SEED | 基因递送三岔路:AAV、LNP、EV 怎么选 SEED | AAV, LNP or EV: choosing the delivery platform AI-assisted · reviewed
University of Texas MD Anderson Cancer Center、Peking University Shenzhen Graduate School 和 Shenzhen Bay Laboratory 的 Yifan Ma 与 Andrew S. Lee、Wen Jiang、Betty Y. S. Kim 团队近期撰写的 Review 梳理了新兴基因递送平台中 AAV、LNP 和 EV 的工程挑战与转化机会,为判断哪一种递送平台适合哪一种 gene therapy 问题提供了一张更清晰的领域地图。
这篇 Review 试图回答什么问题?
这篇 Review 问的是一个基因治疗转化里非常实际的问题:当 payload 可以是 DNA、mRNA、siRNA、saRNA、RNP、base editor、prime editor 或 CAR/TCR 组件时,递送平台到底应该怎么选?
过去讨论 gene delivery 时,AAV、LNP 和 EV 往往被放在不同语境里:AAV 是最成熟的病毒载体,LNP 是 mRNA 药物和体内编辑的非病毒平台,EV 则被看作更天然、更低免疫原性的下一代载体。问题是,临床项目不能只问“哪个平台更先进”,而要问:payload 多大、表达要多久、靶组织在哪里、能否重复给药、制造能否放大、监管路径是否清楚、免疫风险是否可控。
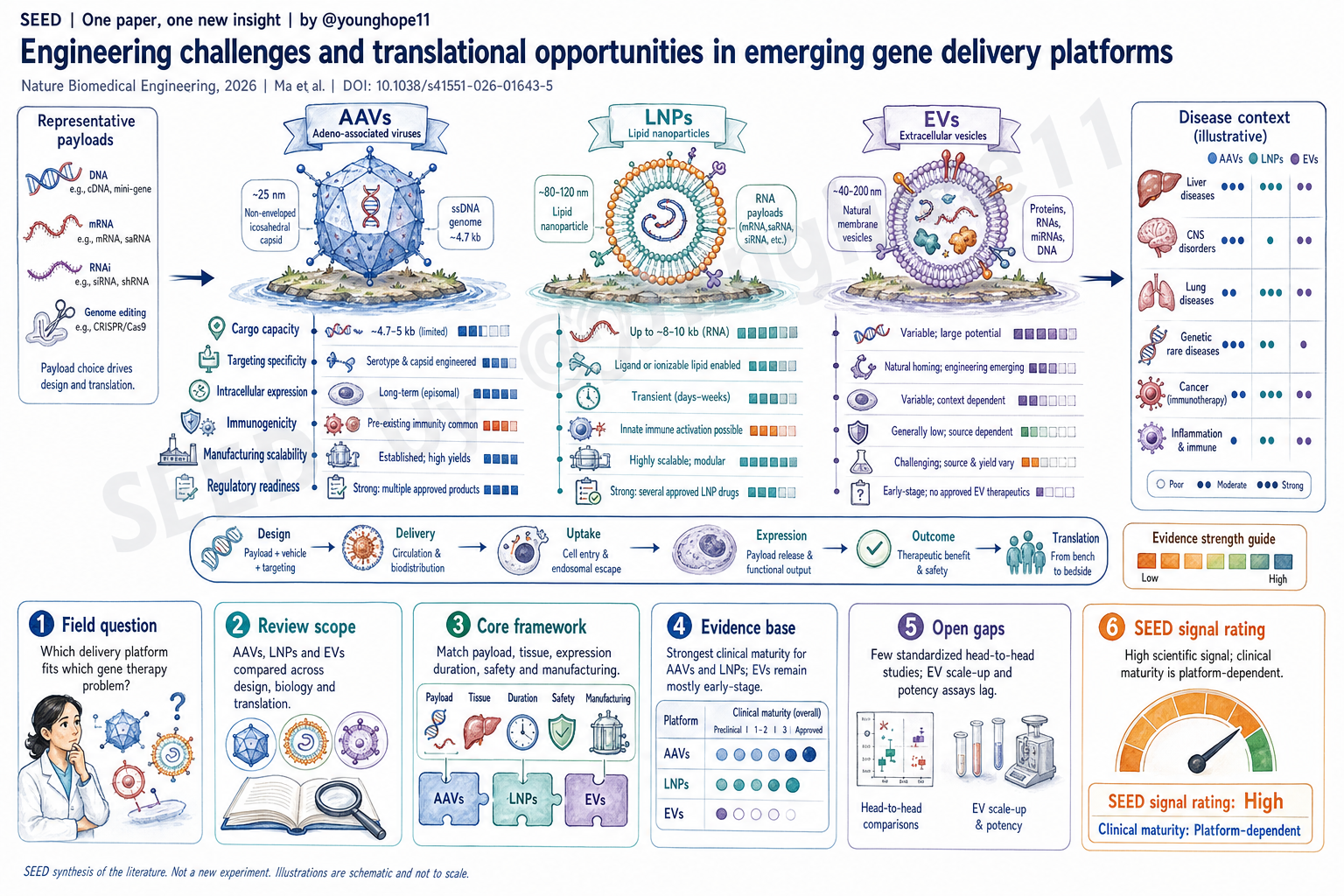
因此,这篇综述的核心价值不是宣布 AAV、LNP 或 EV 的单一胜者,而是把三类平台放在 cargo compatibility、targeting specificity、intracellular expression、biological tolerability、GMP manufacturing、formulation stability、regulatory readiness 和 disease context 这些维度上横向比较。
它真正整理出的新框架是什么?
它整理出的框架可以概括为一句话:不要按平台信仰选载体,要按 payload、组织、表达时长、安全边界和制造成熟度来匹配平台。
AAV 的位置最清楚:适合小型 DNA payload 和需要较长表达窗口的场景,临床和制造经验最成熟,已经有多个获批产品;但它被约 4.7 kb 的包装容量、预存中和抗体、高剂量免疫毒性、难以重复给药和长期安全监测限制。对 DMD、large editor 或需要可逆表达的项目,AAV 天然吃亏。
LNP 的优势是模块化、可规模化、可装载多种核酸,尤其适合 mRNA、siRNA、saRNA、编辑器 mRNA 加 guide RNA 或 RNP 这类 transient payload。它的临床证明来自 Onpattro 和 mRNA 疫苗,并正在延伸到体内基因编辑。但 LNP 默认偏肝脏,内体逃逸效率低,表达多为短暂,重复给药时还要管理先天免疫、anti-PEG 或 lipid-associated reactogenicity。
EV 的吸引力来自天然膜结构、低免疫原性、潜在屏障穿越和组织归巢能力,特别适合 CNS、肺、肿瘤微环境、免疫调控等难递送场景。但 EV 的短板也最硬:cargo loading 低,异质性高,活性成分定义不清,GMP 放大、纯化、potency assay 和监管分类都还不成熟。
这篇 Review 还把 hybrid delivery 放进框架里:EV-associated AAV、LNP-EV hybrid、virus-lipid hybrid 等路线不是为了追求概念复杂,而是试图把 AAV 的表达效率、LNP 的载荷能力和 EV 的免疫/屏障优势组合起来。问题在于,hybrid 往往同时继承制造复杂性、低产率、杂质控制和监管不确定性。
证据链强在哪里?
强在它把平台工程、临床进展和制造监管放在同一个判断系统里,而不是只比较某一个体外指标。
在 cargo 维度上,文章给出的差异很有操作性:AAV 适合约 4.7 kb 以内的 ssDNA payload;LNP 可高效封装 1-5 kb mRNA,saRNA 这类 9-12 kb 结构在优化后也能达到较高效率;EV 可以天然携带小 RNA,但长 mRNA 和编辑组件的装载仍然低效。对 base editor、prime editor、DMD microgene 或多组件编辑系统来说,这个维度本身就会决定很多平台选择。
在功能维度上,文章把“能不能到组织”和“到细胞后能不能表达”拆开看。AAV 的 capsid tropism 和工程化工具最成熟;LNP 的选择性器官递送正在通过 lipid chemistry、charge、size、ligand 和 administration route 改进;EV 有天然 homing 和 barrier-crossing 潜力,但也容易被肝脾清除。进入细胞后,AAV 的内体逃逸和核进入支持长期表达,LNP 的 cargo release 只有约 1-2% 这一瓶颈很关键,而 EV 的内体逃逸可能更强,但表达一致性又被低 loading 和异质性限制。
在临床成熟度上,证据最强的是 AAV 和 LNP。AAV 已经在 Luxturna、Zolgensma、Hemgenix、Roctavian、Elevidys、Beqvez、Upstaza 等产品中证明了临床可行性。LNP 则从 Onpattro、COVID-19 mRNA vaccine 走到体内编辑和免疫治疗方向,文章提到 NTLA-2001 可在患者中带来高幅度 TTR protein reduction,NTLA-2002 也显示出强 kallikrein B1 knockdown。相比之下,EV 目前更多处在 preclinical 和 early clinical 阶段,还没有获批 EV gene therapy。
在制造和监管维度上,文章也没有只讲科学潜力。AAV 和 LNP 已有相对清楚的 CQA、纯化和监管路径;EV 的 donor cell source、vesicle subtype、cargo identity、batch variability、potency assay 和 contamination control 仍是系统性难题。这一点对于真正做药的人比“哪个平台更酷”更重要。
最大局限是什么?
最大局限是这仍然是一篇叙述性 Review,而不是严格意义上的 systematic review 或 meta-analysis。它的框架很有用,但不同平台的证据来自不同 payload、疾病、给药路径、剂量、动物模型和临床阶段,不能被直接读成公平的 head-to-head 排名。
文章自己也指出,AAV、LNP 和 EV 之间真正标准化的头对头比较很少。很多比较会因为 formulation 不等价、active pharmaceutical ingredient 不等价、剂量换算不等价、给药路线不同或研究者平台偏好而产生偏差。因此,表格里的强弱评分适合做方向判断,不适合替代具体项目中的实验证据。
第二个局限是领域变化太快。AAV capsid engineering、selective organ targeting LNP、AI-guided lipid design、EV loading、EV-LNP hybrid、in vivo CAR delivery 和体内编辑项目都在快速推进。综述给的是 2026 年当下的领域地图,但某些平台成熟度可能会很快被新的临床数据改写。
第三个局限是 EV 的证据基础还不够稳。EV 的天然屏障穿越和低免疫原性非常诱人,但很多结论仍依赖 preclinical model;活性成分、剂量单位、载荷效率、纯化标准、储存稳定性和 potency assay 没有统一,导致不同研究之间可比性不足。
对转化或领域判断有什么意义?
它的转化意义在于提供了一个“平台选择清单”。如果项目需要长期表达、小 DNA payload,并且可以接受单次给药和免疫管理,AAV 仍然是最成熟选项。如果项目需要大 RNA、编辑器、可逆表达、可重复给药或快速迭代,LNP 更像默认起点,尤其是肝脏、代谢病、疫苗和部分体内编辑场景。如果项目面对 BBB、肺、肿瘤基质、免疫调控或需要低免疫原性的局部/屏障场景,EV 值得关注,但目前更适合作为探索性平台或 hybrid 组件,而不是最稳的临床主力。
更重要的是,这篇 Review 把“递送”从单一效率问题变成了系统工程问题。一个平台能不能转化,不只看转染率,还要同时看 biodistribution、endosomal escape、payload expression duration、repeat dosing、immunogenicity、manufacturing yield、batch consistency、cold-chain stability、regulatory category 和 cost。
对下一步研发来说,它也给出明确任务:需要标准化 head-to-head comparison;需要把 age、sex、metabolic state、immune status 等患者变量纳入平台选择;需要用 multi-omics、high-resolution imaging 和 AI formulation tools 来建立更可预测的 delivery design;还需要让 EV 和 hybrid platform 尽快形成可监管的 CQA 与 potency assay。
Yang 的信号评级:High
理由:这篇 Review 的科学信号很强,因为它没有把 gene delivery 写成平台宣传,而是把 AAV、LNP 和 EV 放进同一套工程和转化约束里比较。它最有价值的地方,是把 payload、组织、表达时长、免疫风险、制造放大和监管成熟度串成一个可用于项目判断的框架。
我会把它评为科研信号 High。它不是新实验论文,所以 High 不来自某个单一数据点,而来自领域整理的质量:文章能帮助读者更清楚地区分“科学上有潜力”“工程上可实现”和“临床上已成熟”这三件事。
但这个 High 是“科研信号 High”,不是“所有平台临床就绪 High”。临床成熟度我会单独评为 Platform-dependent:AAV 和 LNP 已有较强临床与监管基础,但适应症和风险边界不同;EV 的生物学吸引力很高,临床成熟度仍偏 Low;hybrid platform 则还需要证明复杂性真的能换来足够大的转化收益。
Yifan Ma and the team of Andrew S. Lee, Wen Jiang and Betty Y. S. Kim at the University of Texas MD Anderson Cancer Center, Peking University Shenzhen Graduate School and Shenzhen Bay Laboratory recently wrote a Review that maps the engineering challenges and translational opportunities of AAVs, LNPs and EVs as emerging gene delivery platforms, offering a clearer field map for matching delivery systems to gene therapy problems.
What question does this review try to answer?
This review asks a very practical question for gene therapy translation: when the payload may be DNA, mRNA, siRNA, saRNA, RNPs, base editors, prime editors or CAR/TCR components, how should the delivery platform be chosen?
AAVs, LNPs and EVs are often discussed in different contexts. AAVs are the most mature viral vectors. LNPs are the non-viral platform behind mRNA medicines and many in vivo editing programs. EVs are viewed as a more natural and potentially less immunogenic next-generation carrier. But a clinical program cannot ask only which platform is newer or more exciting. It has to ask how large the payload is, how long expression should last, where the target tissue is, whether repeat dosing is needed, whether manufacturing can scale, whether the regulatory path is clear and whether immune risk can be controlled.
The value of this review is therefore not that it crowns AAV, LNP or EV as the single winner. It compares the three platforms across cargo compatibility, targeting specificity, intracellular expression, biological tolerability, GMP manufacturing, formulation stability, regulatory readiness and disease context.
What framework does it synthesize?
The synthesized framework can be summarized simply: choose the vector by payload, tissue, expression duration, safety boundary and manufacturing maturity, not by platform preference.
AAV has the clearest position. It fits small DNA payloads and settings that need a longer expression window, and it has the deepest clinical and manufacturing experience, with multiple approved products. But it is constrained by an approximately 4.7 kb packaging limit, pre-existing neutralizing antibodies, high-dose immune toxicity, limited repeat dosing and long-term safety monitoring. For DMD, large editors or applications that need reversible expression, AAV begins at a disadvantage.
LNPs offer a modular and scalable way to deliver diverse nucleic acids, especially transient payloads such as mRNA, siRNA, saRNA, editor mRNA plus guide RNA or RNPs. Their clinical proof comes from Onpattro and mRNA vaccines, and they are now extending into in vivo genome editing. However, LNPs default toward liver delivery, have poor endosomal escape, usually produce transient expression and require management of innate immunity, anti-PEG responses or lipid-associated reactogenicity during repeated dosing.
EVs are attractive because of their natural membrane structure, low immunogenicity, potential barrier crossing and tissue-homing properties, especially for hard-to-reach settings such as the CNS, lung, tumor microenvironment and immune regulation. But their weaknesses are also substantial: low cargo loading, high heterogeneity, poorly defined active ingredients, difficult GMP scale-up, challenging purification, immature potency assays and uncertain regulatory classification.
The review also places hybrid delivery systems within the same framework. EV-associated AAVs, LNP-EV hybrids and virus-lipid hybrids are not complexity for its own sake. They try to combine AAV expression efficiency, LNP payload capacity and EV immune or barrier advantages. The hard question is whether these hybrids can avoid inheriting manufacturing complexity, low yield, impurity control problems and regulatory uncertainty.
Where is the evidence base strongest?
The evidence base is strongest where the article connects platform engineering, clinical progress and manufacturing regulation within the same decision system, instead of comparing only one in vitro metric.
For cargo, the distinctions are actionable. AAVs fit ssDNA payloads of roughly 4.7 kb or less. LNPs can efficiently encapsulate 1-5 kb mRNA, and optimized formulations can support larger 9-12 kb saRNA constructs with relatively high efficiency. EVs naturally carry small RNAs, but efficient loading of longer mRNAs and editing components remains difficult. For base editors, prime editors, DMD microgenes or multi-component editing systems, this axis alone can strongly shape platform choice.
For function, the review separates tissue access from intracellular expression. AAVs have the most mature capsid tropism and engineering toolkit. LNP selective organ delivery is being improved through lipid chemistry, charge, size, ligands and administration route. EVs have natural homing and barrier-crossing potential but are also prone to liver and spleen clearance. After cell entry, AAV endosomal escape and nuclear delivery support durable expression. LNPs face a major cargo-release bottleneck of roughly 1-2%. EVs may escape endosomes more effectively, but expression consistency is limited by low loading and heterogeneity.
For clinical maturity, the strongest evidence sits with AAVs and LNPs. AAVs have demonstrated clinical feasibility through products such as Luxturna, Zolgensma, Hemgenix, Roctavian, Elevidys, Beqvez and Upstaza. LNPs have moved from Onpattro and COVID-19 mRNA vaccines toward in vivo editing and immunotherapy; the review discusses examples such as NTLA-2001, which achieved large transthyretin protein reduction in patients, and NTLA-2002, which showed strong kallikrein B1 knockdown. EVs, by contrast, remain mostly preclinical or early clinical, with no approved EV gene therapy.
The manufacturing and regulatory discussion is also a strength. AAVs and LNPs have relatively defined CQAs, purification workflows and regulatory expectations. EVs still face systemic problems around donor cell source, vesicle subtype, cargo identity, batch variability, potency assays and contamination control. For drug developers, that may matter more than which platform sounds more biologically elegant.
What is the biggest limitation?
The biggest limitation is that this is still a narrative review, not a formal systematic review or meta-analysis. Its framework is useful, but the evidence for each platform comes from different payloads, diseases, administration routes, doses, animal models and clinical stages. It should not be read as a fair head-to-head ranking.
The article itself emphasizes that truly standardized head-to-head comparisons among AAVs, LNPs and EVs are scarce. Many comparisons can be biased by non-equivalent formulations, different active pharmaceutical ingredients, unmatched dose metrics, different routes of administration or investigator preference for a particular platform. The scoring tables are useful for directional judgment, but they cannot replace project-specific experimental evidence.
A second limitation is that the field is moving quickly. AAV capsid engineering, selective organ targeting LNPs, AI-guided lipid design, EV loading, EV-LNP hybrids, in vivo CAR delivery and in vivo editing programs are all advancing rapidly. The review provides a 2026 field map, but clinical maturity for some platforms may be rewritten by new data.
A third limitation is that the EV evidence base remains less stable. EV barrier crossing and low immunogenicity are appealing, but many claims still rely on preclinical models. Active ingredient definition, dose units, loading efficiency, purification standards, storage stability and potency assays remain insufficiently standardized, limiting comparability across studies.
What does it mean for translation or field-level judgment?
Its translational value is that it gives the field a platform-selection checklist. If a program needs long-term expression, a small DNA payload and can accept single dosing plus immune management, AAV remains the most mature option. If the program needs a large RNA, an editor, reversible expression, repeat dosing or rapid iteration, LNP is often the default starting point, especially for liver, metabolic disease, vaccines and some in vivo editing settings. If the target involves the BBB, lung, tumor stroma, immune modulation or a local/barrier context where low immunogenicity matters, EVs deserve attention, but today they are better viewed as exploratory platforms or hybrid components than as the most reliable clinical workhorse.
More importantly, the review reframes delivery as a systems engineering problem rather than a single efficiency metric. Whether a platform can translate depends not only on transfection rate, but also on biodistribution, endosomal escape, payload expression duration, repeat dosing, immunogenicity, manufacturing yield, batch consistency, cold-chain stability, regulatory category and cost.
For future work, the review also defines the next experiments clearly: standardized head-to-head comparisons are needed; patient variables such as age, sex, metabolic state and immune status should be integrated into platform choice; multi-omics, high-resolution imaging and AI formulation tools should make delivery design more predictable; and EV and hybrid platforms need regulator-ready CQAs and potency assays.
Yang’s signal rating: High
Reason: the scientific signal of this review is strong because it does not treat gene delivery as platform marketing. It compares AAVs, LNPs and EVs within the same engineering and translational constraints. Its most useful contribution is connecting payload, tissue, expression duration, immune risk, manufacturing scale-up and regulatory maturity into a framework that can guide project-level judgment.
I would rate the scientific signal as High. This is not an original experimental paper, so the High does not come from one decisive dataset. It comes from the quality of the field synthesis: the review helps readers separate scientific potential, engineering feasibility and clinical maturity.
But this High means scientific signal High, not clinical readiness High for every platform. I would rate clinical maturity as platform-dependent: AAVs and LNPs already have stronger clinical and regulatory foundations, although their disease fit and risk boundaries differ; EVs are biologically attractive but still clinically Low in maturity; hybrid platforms still need to prove that their added complexity yields enough translational benefit.