SEED | 在体 CRISPR 第一次把 HAE 推到 III 期证据 SEED | In vivo CRISPR reaches phase 3 disease control in HAE AI-assisted · reviewed
Danny M. Cohn、Padmalal Gurugama 与 HAELO Investigators 团队近期报道,单次静脉输注 lonvoguran ziclumeran 可在 C1 inhibitor deficiency 型遗传性血管性水肿患者中显著降低发作频率,为非肝脏遗传病通过肝靶向在体 CRISPR 改变疾病通路提供了新的临床证据。
HAE 的关键不是补 C1-INH,而是压住 kallikrein 通路
这篇论文讨论的是 hereditary angioedema due to C1 inhibitor deficiency。疾病机制上,SERPING1 相关 C1 inhibitor 不足或功能异常会导致 kallikrein-kinin 通路失控,bradykinin 过量,最终造成反复、不可预测、甚至危及生命的水肿发作。
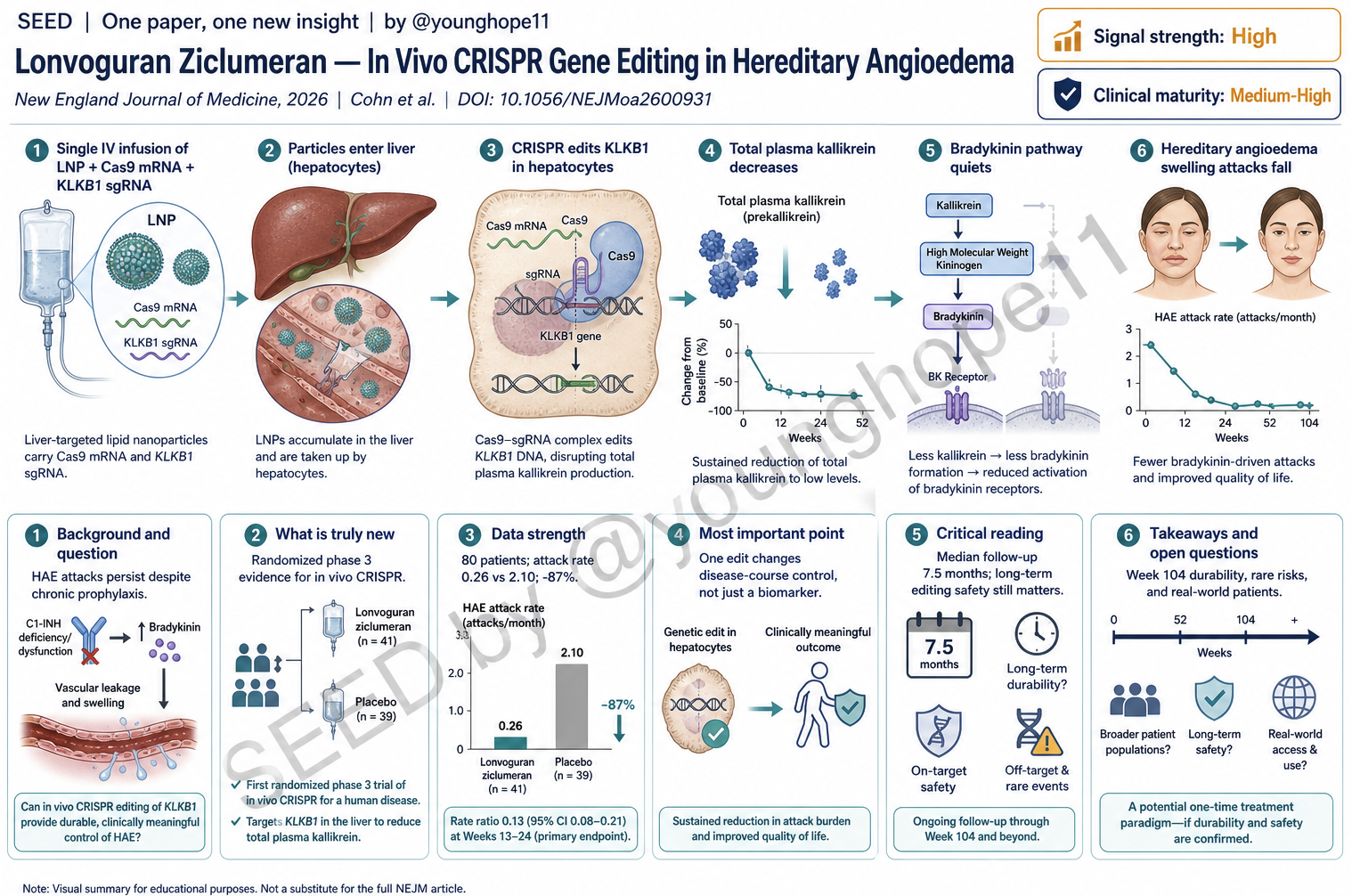
Lonvo-z 的策略不是补充 C1-INH,也不是周期性阻断 kallikrein,而是用脂质纳米颗粒把 CRISPR-Cas9 组件送入肝细胞,靶向编辑 KLKB1,降低 prekallikrein/total plasma kallikrein。核心问题是:一次性在体编辑能否在随机 III 期试验里真正减少 HAE 发作,同时短期安全性可接受。
新意在于把“一次性编辑”推进到随机 III 期
研究设计是 HAELO,跨国、双盲、随机、安慰剂对照 III 期试验。80 名至少 16 岁、C1 inhibitor deficiency 型 HAE 患者按 2:1 随机接受单次 50 mg lonvo-z 静脉输注或 placebo;主要终点是输注后第 5 周到第 28 周的 investigator-confirmed monthly attack rate。
真正的新意有两层。第一,它是一个 in vivo CRISPR 药物在明确临床终点上的随机对照证据,而不是早期单臂降 biomarker。第二,它把一个肝源性可调控通路 KLKB1 变成 HAE 的长期病程控制入口,显示“一次性降低病理通路输入”可能替代长期预防给药。
数据强在临床终点、药效标志物和患者报告结果一致
主要结果很清楚:第 5-28 周,lonvo-z 组 LS mean monthly attack rate 为 0.26,placebo 组为 2.10,相对差异 -87%,P<0.001。需要按需治疗的发作率相对降低 -89%,中重度发作率相对降低 -91%。
更重要的是,临床改善不是只体现在均值上。第 5-28 周完全无发作的患者比例为 32/52,即 62%,而 placebo 为 3/28,即 11%。AE-QoL 总分从基线到第 28 周的改善也明显更大:lonvo-z 为 -23.51,placebo 为 -6.47,组间差 -17.04,超过 6 分的最小临床重要差异。
药效标志物也支持机制闭环。total plasma kallikrein 在第 2 周已平均下降 65%,第 5 周达到稳态,维持到随访末;第 28 周报告的平均下降约为 82%。这让临床终点和 KLKB1/kallikrein 机制之间形成较紧的连接。
最重要的一点:这是临床病程控制,不只是编辑成功
这篇文章的核心价值不是“CRISPR 又能编辑一个基因”,而是一次性编辑在真实临床发作终点上超过 placebo,并且在生活质量上同步改善。对在体基因编辑领域来说,这比单纯报告血液 biomarker 更重要。
它也说明了一个可复制的药物开发逻辑:选择肝脏产生、部分降低即可获益、完全缺失在人类中相对可耐受的靶点,再用短暂暴露的 LNP-Cas9 系统做持久通路重设。KLKB1 比很多组织内必需基因更适合成为早期在体编辑靶点。
批判性阅读:III 期很强,但长期编辑风险还没有结束
安全性短期表现不错,但不能把它读成长期安全已定论。day 1 到 week 28,lonvo-z 组任何不良事件 92%,placebo 组 86%;lonvo-z 组无 serious adverse event,也无 grade 3 或更高级别事件。最常见问题是 infusion-related reaction,lonvo-z 组 62%,placebo 组 18%,多为 1-2 级、短暂。
需要继续看的点有三个。第一,随访中位数只有 7.5 个月,基因编辑药物的长期肝脏安全、off-target、clonal expansion 和免疫反应需要更长观察。第二,药企资助和医学写作参与需要在解读时记住,虽然随机对照设计降低了主要疗效偏倚。第三,患者数仍有限,无法充分覆盖共病、肝病、特殊人群和长期 kallikrein 缺乏的罕见风险。
对在体编辑的启发:好靶点比炫技术更重要
后续最值得追的问题不是“能不能再编辑更多基因”,而是怎样选择类似 KLKB1 的靶点:肝脏可递送、靶点降低有明确药理学、长期部分缺失相对可承受、临床终点可在合理时间内读出。
对 HAE 本身,关键是 week 104 的长期疗效和安全性、anti-Cas9/anti-drug antibodies 的长期意义、是否可在更广泛患者中保持攻击率降低,以及一次性编辑相对现有长期预防药物的风险收益边界。
Yang 的信号评级:High
轴一,信号强度:High。理由:随机 III 期、临床发作终点、生活质量和 kallikrein 药效标志物方向一致,且效应量很大。
轴二,临床成熟度:Medium-High。理由:III 期证据已经很强,但这是持久性在体编辑,长期安全性、罕见风险和更广泛真实世界人群仍需要随访。
一句话总结:这篇论文把在体 CRISPR 从“能不能编辑”推进到“能不能改变患者发作病程”的临床层面。
Danny M. Cohn, Padmalal Gurugama, and the HAELO Investigators recently reported that a single intravenous infusion of lonvoguran ziclumeran markedly reduced attack frequency in patients with C1 inhibitor deficiency hereditary angioedema, providing new clinical evidence that liver-targeted in vivo CRISPR can reset a disease-driving pathway beyond the liver.
The key HAE lever is kallikrein pathway pressure
The disease context is hereditary angioedema due to C1 inhibitor deficiency. Pathogenic SERPING1 biology leads to dysregulated kallikrein-kinin signaling, excess bradykinin, and recurrent unpredictable swelling attacks that can be debilitating or life-threatening.
Lonvo-z does not replace C1 inhibitor and does not require repeated kallikrein blockade. It uses lipid nanoparticles to deliver CRISPR-Cas9 components to hepatocytes and edit KLKB1, lowering prekallikrein and total plasma kallikrein. The central question is whether one-time in vivo editing can reduce HAE attacks in a randomized phase 3 trial with acceptable short-term safety.
The novelty is one-time editing with randomized phase 3 evidence
HAELO was a multinational, double-blind, randomized, placebo-controlled phase 3 trial. Eighty patients at least 16 years old with C1 inhibitor deficiency HAE were randomized 2:1 to a single 50 mg intravenous infusion of lonvo-z or placebo. The primary endpoint was investigator-confirmed monthly attack rate from week 5 through week 28.
The novelty has two layers. First, this is randomized controlled evidence for an in vivo CRISPR therapy on a clinical endpoint, not just an early single-arm biomarker result. Second, it turns a liver-derived pathway component, KLKB1, into a durable disease-control entry point for HAE.
The strongest data connect attacks, quality of life, and pharmacodynamics
The primary result is strong: from week 5 through week 28, the least-squares mean monthly attack rate was 0.26 with lonvo-z and 2.10 with placebo, a relative difference of -87% with P<0.001. Attacks requiring on-demand therapy fell by -89%, and moderate or severe attacks fell by -91%.
The effect was also clinically visible at the patient level. Attack-free status from week 5 through week 28 occurred in 32 of 52 patients, or 62%, in the lonvo-z group versus 3 of 28, or 11%, in the placebo group. AE-QoL improved more with lonvo-z: -23.51 versus -6.47 points, a between-group difference of -17.04 points, exceeding the 6-point minimal clinically important difference.
The pharmacodynamic readout supports the mechanism. Total plasma kallikrein fell by a mean of 65% by week 2, reached steady state by week 5, and was maintained through follow-up; the reported week 28 mean reduction was about 82%. Clinical attack reduction and pathway suppression therefore point in the same direction.
The important point is disease-course control, not just editing
The central value is not that CRISPR can edit another gene. It is that one-time editing improved real attack outcomes versus placebo and improved quality of life in parallel. For the in vivo editing field, that is more meaningful than showing a blood biomarker alone.
It also illustrates a drug-development logic that may be reusable: choose a liver-derived target where partial lowering is therapeutically useful, human deficiency biology is relatively tolerable, and a short-lived LNP-Cas9 exposure can create durable pathway suppression.
Critical reading: strong phase 3 data, unfinished long-term risk
Short-term safety looked favorable, but long-term safety is not settled. From day 1 through week 28, any adverse event occurred in 92% of lonvo-z patients and 86% of placebo patients. There were no serious adverse events and no grade 3 or higher adverse events in the lonvo-z group. The most common issue was infusion-related reaction, 62% with lonvo-z versus 18% with placebo, usually grade 1-2 and transient.
Three caveats matter. The median follow-up was 7.5 months, which is short for a durable gene-editing therapy. The study was industry funded, although the randomized design strengthens the primary efficacy finding. The cohort remains limited for rare long-term liver, off-target, clonal, immune, comorbidity, and lifelong kallikrein-lowering questions.
What this should trigger next
The next question is not simply whether more genes can be edited. It is how to choose targets like KLKB1: liver-deliverable, pharmacologically validated, tolerable when partially reduced, and linked to a clinical endpoint that can be read within a practical trial window.
For HAE, the key next evidence will be week 104 durability and safety, the long-term meaning of anti-Cas9 and anti-drug antibodies, performance in broader patient populations, and the risk-benefit comparison against existing long-term prophylaxis.
Yang’s signal rating: High
Signal strength: High. The randomized phase 3 clinical endpoint, quality-of-life data, and kallikrein pharmacodynamics align, with a large treatment effect.
Clinical maturity: Medium-High. Phase 3 evidence is strong, but durable in vivo editing still requires longer follow-up for rare and delayed risks.
One-sentence summary: This paper moves in vivo CRISPR from “can it edit?” to “can it alter the clinical course of attacks?”